Antibiotics were a revolutionary discovery in the 1920s and by the 1940s, when they had been developed for civilian use, they were the saviour of many, as the message in the poster here makes clear.
But antibiotics have been overused and prescribed inappropriately - in agriculture as well as medicine - all over the world:
- In the UK, a Public Health England report found that 51% of patients were inappropriately prescribed an antibiotic by their GP for coughs and colds, for which antibiotics are ineffective.
- In the US, there are over 22 million inappropriate antibiotic prescriptions made for acute respiratory infections each year out of a total of 44 million antibiotic prescriptions - meaning 50% are inappropriate.
- In Australia, the 2013 National Antimicrobial Prescribing survey found that around 30% of antibiotic prescriptions are inappropriate.
- China has the highest antibiotic prescription rates in the world - one study found that 2 in 3 patients visiting clinics with only mild cold or flu symptoms received inappropriate prescriptions for antibiotics, with many patients prescribed powerful “second-line” antibiotics that are supposed to be reserved for serious illnesses.
So many unnecessary prescriptions have meant bacteria are becoming increasingly resistant to antibiotics, creating situations where patients are now dying due to bacterial infections which cannot be treated by any antibiotic.
For example, in April 2015 in China, a 3 year old boy visited a hospital for abdominal pain that was then diagnosed as colitis. He died three weeks later from organ failure induced by Klebsiella pneumoniae—a superbug resistant to antibiotics. The UK Review on Antimicrobial Resistance has forecast that resistance will result in 10 million deaths and $100 trillion in unachieved GDP a year by 2050.
Dame Sally Davies, Chief Medical Officer for the UK and a prominent campaigner on the issue maintains:
"Antimicrobial resistance poses a catastrophic threat. If we don’t act now, any one of us could go into hospital in 20 years for minor surgery and die because of an ordinary infection that can’t be treated by antibiotics. And routine operations like hip replacements or organ transplants could be deadly because of the risk of infection."
So given this scary behavioural challenge, can we curtail inappropriate use of antibiotics in primary care using interventions inspired by behavioural science?
Basic education, efforts to increase awareness and financial incentives have had only a small effect. So a team of researchers from the University of Southern California in LA tested a number of different interventions on primary care physicians in 49 practices in Boston and LA, based around socially motivated behaviours. Two of these interventions were astoundingly successful, reducing prescription rates by around 16 - 18 percentage points. As the lead researcher on the study, Jason Doctor says -
"It turns out doctors are humans too; just like others, they respond to the social cues that others do."
Below we describe these two interventions:
INTERVENTION 1: PEER COMPARISON
INTERVENTION 1: PEER COMPARISON
Doctors in this intervention received an email telling them of their performance ranking for inappropriate prescribing.
- Doctors with the lowest prescription rates were told they were a 'top performer' and received a 'Congratulations' message.
- Doctors with poorer performance received an email with a count of their inappropriate antibiotic prescribing. (see image)
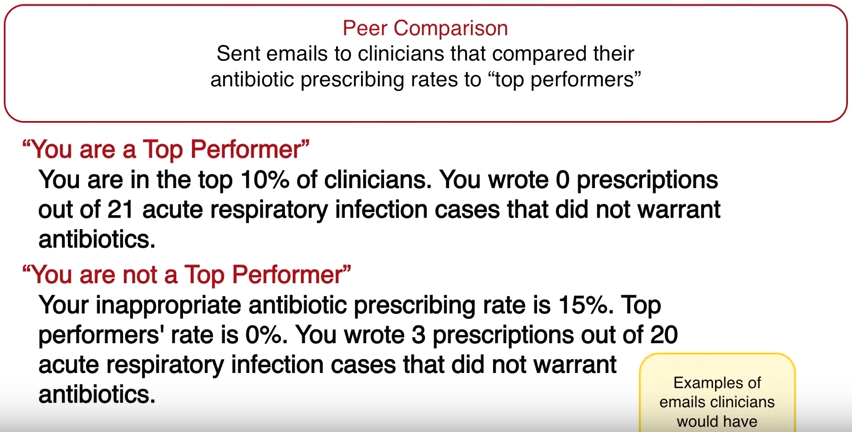
This intervention made clever use of descriptive social norms – defined as what other doctors are doing - realigning doctors' misperceptions of prescription rate norms and practices. There is also a strong element of 'big brother' - making doctors fully aware their prescription patterns are being observed...
This intervention led to a 16 percentage point reduction in antibiotic prescriptions for acute respiratory infections by these doctors, from 20% down to 4%.
INTERVENTION 2: ACCOUNTABLE JUSTIFICATION
INTERVENTION 2: ACCOUNTABLE JUSTIFICATION
If a doctor in this intervention began to register an antibiotic prescription for a patient in their electronic file, an automatic prompt would appear, asking the doctor to note down the reasons why antibiotics were justified in this case (see image).
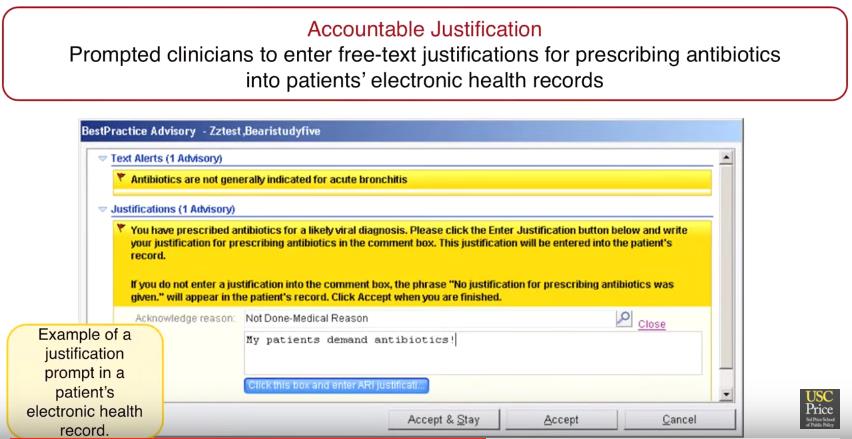
This written note would then be recorded in the patient's file and accessible for other doctors and healthcare professionals to see. However, the doctor could also change their mind and cancel the prescription.
The prompt likely made injunctive social norms (practices doctors knew they should be doing) and professional conduct far more salient in a timely manner, perhaps making it easier to resist pressure from their patient to be prescribed antibiotics. Such pressure is thought to be one of the main drivers of inappropriate prescribing due to patient ignorance of when antibiotics are effective - and not effective.
The prospect of a written record likely enhanced this social effect, as doctors realised their justification (or lack of one) would be on their file for others to see and record.
This intervention led to an 18 percentage point reduction in antibiotic prescriptions for acute respiratory infections by doctors, from 23% to 5%.
Conclusion
These findings are incredibly encouraging, demonstrating the considerable power of behavioural science when it is used well. Whilst we should never neglect or dismiss other ways of changing behaviour such as regulation or policy change, when simple, low cost messaging can lead to such significant changes in behaviour, choosing to use behavioural science is a ‘no-brainer’.
Read more from Crawford Hollingworth in our Cluhouse.